
Nose shapes

The outline of the nose is often perceived as disturbing the overall expression of the face when the nose is the dominating feature of the face. A pronounced misshape of the nose becomes a "negative eye-catcher" in your face that you' d like to have changed. Furthermore, some nose shapes may impair the functionality of the nose, e.g. breathing or smelling.
Our ambition is to achieve a natural looking nose that fits your face while improving or maintaining its function and thereby enhancing your overall sense of well-being and self-confidence. The outer shape of the nose demonstrates
numerous variations, and approximately 250 different nose types have been identified until now.
The most common categories are:
Hump nose

An attractive nasal bridge is usually straight, with the exception of the female nasal bridge, which may be slightly curved inwards. When a nasal bridge is more strongly curved outwards, it is referred to as a hump nose.
This is most commonly genetic, but may also result from trauma, coupled with unproportional growth. In some cases, you can even sense the cartilage or bone fragments underneath the skin.
A small hump of approx. 0.3 mm is tolerable and gives the nose a natural appearance since it occurs quite frequently.

Correction of a hump nose
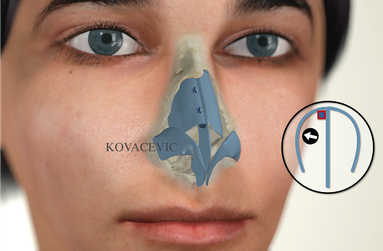
The removal of the hump is often combined with the subsequent reconstruction of the nasal bridge, as the so-called collapse of the nasal bridge can otherwise occur, whereby the lateral cartilages migrate backwards and form an image of the inverted letter "V" - see picture on the right.
Example of a pre-operated nose with the so-called "Inverted- V" / reverse V appearance. There had been no reconstruction of the nasal bridge performed in the patient, therefore a massive change in the shape occurred.
The reconstruction is carried out either by means of cartilaginous strips (the so-called spreader grafts, picture 1), which are obtained from the nasal septum, or the lateral cartilage is shifted inwards and thus a new nasal bridge is constructed (the so-called spreader flaps, picture 2).


In some cases, where a nose hump appears very symmetrical, the so-called nasal bridge preservation technique (dorsal preservation technique, let down) is applied. In the process, the nose's own bridge is preserved and shifted inwards.
Crooked nose

In order to obtain the so-called facial axis, a line is drawn between the point in the middle of the eyebrows and the point in the middle of the upper lip. If there is a significant deviation of more than 5° from this line, the nose is considered to be crooked.
On the other hand, many people have facial asymmetry, so that sometimes the nose is surgically placed in the middle, but the face appears even more asymmetrical. Therefore, a joint facial analysis is essential to decide on where exactly the nose should be positioned. Sometimes the geometrically perfect position is a disadvantage. A crooked nose is often associated with a crooked nasal septum, which partially displaces one half of the inner nose, causing nasal respiratory obstruction.
Correction of a crooked nose
The correction of a crooked nose always goes hand in hand with a correction of the nasal septum, which serves as the basic pillar of the nose. The formation of a crooked nose is very often the result of trauma, even in early childhood, and it is usually accompanied by a hump. In rare cases of some patients, it is exclusively a cartilaginous crooked nose, where the straightening of the nasal septum plays a decisive role. In the majority of cases, the bony nose is also affected.
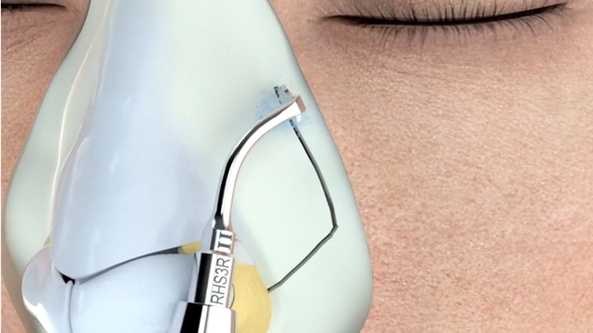
Extreme precision is required in bony incisions when operating on a crooked nose, which is why an ultrasonic scalpel/piezo instrument is employed in the process. In some cases, the bone is significantly thicker on one side; in such patients, the same instrument is used to perform what is known as bone modeling or rhinosculpting. Counterbalancing, cartilaginous grafts are used at the same time.
The grafts are most often obtained from the nasal septum, but in some cases also from the auricle or rib cartilage. These add extra volume to one side of the nose so that it appears visually straight.
Asymmetry of the nostrils
In certain cases, there is also an asymmetry of the nostrils, so that surgery is also required in this area. Fortunately, the surgery is often followed by a significant improvement in breathing. One of the risks of surgery on a crooked nose in particularly pronounced cases is that the nose sometimes tries to move back into its former position, for example by pulling on the muscles. Therefore, patients cannot always be promised a perfect, straight nose, instead it is important to clarify that the nose will become significantly "straighter".
Broad nose
Eine Nase kann auch in ihrer knöchern-knorpeliger Basis relativ weit wirken, häufig kombiniert mit einer breiten Nasenspitze.
Diese fast fassförmigen Nasen gehen an der Basis weiter nach außen als die vertikalen Linien, die von den inneren Augenwinkeln senkrecht nach unten gezogen sind.
Die Ursache einer Breitnase kann genetisch sein oder als Folge eines Traumas auftreten.
Correction of a broad nose
The surgeon must consider the thickness of the nasal bones when planning the operation. Very thick bones have the tendency to shift inwards, thus narrowing the airways and causing respiratory obstruction. In these cases, the so-called computed tomography sectional imaging is required for planning of the surgery.
In most cases, the bone can be modeled in such a way that there are no functional impairments later on.
Besides narrowing the nose, an operation on the broad nose must also be aimed at preserving the inner mucous membrane to prevent osseous collapse. Therefore, the ultrasonic scalpel/piezo instrument, which is extremely gentle on the soft tissues, is used in such cases.
These patients also have a very broad nose tip and nose base including nostrils. In many cases, the nose tip also appears to be quite low, so initially it is lengthened by means of a graft from the patient's own cartilage. It acts as a tent pole which provides the tent with shape. The desired effect is usually achieved by removing a small amount of cartilage from the nose tip and shaping it with special sutures.
Skin thickness
In some patients the broad nose usually comes along with thick skin mantle, especially at the tip of the nose. Depending on the skin thickness, various surgical or medicinal measures can be applied to make the nose tip appear even narrower until the desired effect is achieved. In some cases, where the skin is particularly thick, it is not possible to accomplish a petite nose tip. In the case of wide nostrils, excess soft tissue is removed in a wedge shape and sutured back with utmost care.
Saddlenose

The nasal bridge may sink significantly below the normal level following trauma, nasal septum surgery or a hole in the nasal septum, and may develop the appearance of a saddle, particularly in the middle part of the nose.
These patients may also have a crooked nose depending on the underlying cause. The patients also frequently complain of nasal obstruction. A very crooked nasal septum resulting from trauma is very frequently observed in these patients.
Further causes of a saddle nose include previous operations, especially on the nasal septum, and the associated loss of support. Occasionally, an infection caused by haematoma in the nasal septum may result in the loss of cartilage and support.
Correction of a saddle nose
First of all, the nasal septum surgery should be performed and then the necessary reconstruction should be performed in this area. Afterwards, the access to the nasal bridge is established and the amount of missing material on the nasal bridge is assessed.
This profile deficiency must be filled with the body's own transplants. The cartilage for this is extracted from the nasal septum - if still available - or otherwise from the auricle or a rib, processed in a special way and placed in the defect. Small pieces of cartilage are often joined to blood components; this creates a graft that optimally adapts to the underlying tissue.
This operation is very complex and should be performed by highly experienced surgeons.
Bulbous nose

If the nose tip is very broad, both nostril cartilages are clearly visible under the skin and have grown disproportionately large, it is commonly referred to as a bulbous nose or in technical terms as a bulbous nasal tip.
Sometimes the thickness of the patient's skin is responsible for the shape of the nose to a greater extent.
Correction of a bulbous nose
The surgeon must carefully consider how much cartilage really needs to be removed so as not to weaken the cartilaginous structure too much, and what additional manoeuvres coupled with supportive measures are necessary to achieve an aesthetically beautiful nose tip.
Excessive cartilage removal can lead to massive shrinkage of the nostrils, especially in patients with thin skin.
When viewed from the side, they can develop an upward point in the middle of the nose wing, so that they look like a Chinese hat.
Tension nose

A tension nose refers to a nose that has grown too much and the entire nasal pyramid has become too large in consequence.
It is often very narrow and long on the outside, and at the same time the angle between the lateral cartilage and the nasal septum is very small, so that nasal breathing is impaired.
Correction of a tension nose
The surgical objective is to improve breathing by simultaneous shortening of the outer nose; this procedure is often performed with a very good result. If the nose bridge presents a symmetrical shape when viewed from the front, the most frequent method of choice in our practice is dorsal preservation surgery/ Let Down.